Types of Meningitis
There are numerous types of bacteria that can cause bacterial meningitis, the main types include:
Additional information on these specific types of meningitis, as well as rarer types can be found at the Meningitis Research Foundation's website at:
http://www.meningitis.org/disease-info/types-causes/bacterial-meningitis
- Meningococcal
- Pneumococcal
- Haemophilus influenzae b (Hib)
- Group B Streptoccal (GBS)
- Tubercular (TB)
- E.coli
- Listeria
Additional information on these specific types of meningitis, as well as rarer types can be found at the Meningitis Research Foundation's website at:
http://www.meningitis.org/disease-info/types-causes/bacterial-meningitis
Diagnosis
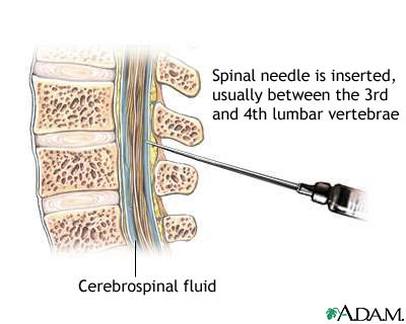
Lumbar puncture procedure [12].
Lumbar puncture
A lumbar puncture is used to collect cerebrospinal fluid (CSF) to determine if meningitis is suspected. However, most often before a lumbar puncture is performed, the clinician will perform a CT scan to ensure there is not a CNS mass lesion or another ailment causing increased intracranial pressure. If the CSF components are consistent with the clinical diagnosis of meningitis, the fluid will most often look cloudy and consistent of the following:
A gram stain is usually performed in conjunction with a lumbar puncture before antimicrobial therapy is started [1].
Determination of Lactate Concentration
Another test used to determine if a patient is infected with bacterial meningitis includes testing for lactate concentration. An important point to note with this test is that it is not performed prior to antimicrobial therapy. A study conducted with 78 patients with acute meningitis determined that all patients had CSF lactate concentrations greater than 4.2 mmol/L. Thus, lactate concentration could be used as a positive discriminative factor for bacterial meningitis with a sensitivity of 96% and a specificity of 100%. However, this test is not widely used to diagnose bacterial meningitis because it does not provide much diagnostic information [2].
Determination of C-reactive protein (CRP) concentration
C-reactive protein (CRP) is produced in the liver and is released six hours after an acute inflammatory reaction, which means CRP could provide a measure of immunity response after infection with meningitis. Patients with meningitis were tested for CRP concentration. Researchers concluded that CRP sensitivity ranged from 69-99% and specificity ranged from 28-99% [3]. However, because of the wide ranges, this measure for confirmed diagnosis is also not widely used.
Determination of procalcitonin concentration
Another measure for meningitis diagnosis might be the presence of procalcitonin. Researchers studied 59 children that had been hospitalized for meningitis and the procalcitonin concentrations were surprisingly high at a concentration greater than 5.0µg/L. The sensitivity of these results was 94% and the specificity was 100%. In adults, the serum concentrations were also tested with concentrations over ng/mL. Both sensitivity and specificity were up to 100% for procalcitonin concentration in adults [4]. These high sensitivity and specificity results provide a positive outlook on using procalcitonin concentration as a diagnosis measure of bacterial meningitis. However, the equipment used to test for procalcitonin concentration is not readily available in clinics, so it is not often used as a diagnostic tool to test for meningitis [4].
A lumbar puncture is used to collect cerebrospinal fluid (CSF) to determine if meningitis is suspected. However, most often before a lumbar puncture is performed, the clinician will perform a CT scan to ensure there is not a CNS mass lesion or another ailment causing increased intracranial pressure. If the CSF components are consistent with the clinical diagnosis of meningitis, the fluid will most often look cloudy and consistent of the following:
- White blood cell count elevated with 1000-5000 cells/mm3
- Glucose concentration less than 40 mg/dL
- Protein concentration
A gram stain is usually performed in conjunction with a lumbar puncture before antimicrobial therapy is started [1].
Determination of Lactate Concentration
Another test used to determine if a patient is infected with bacterial meningitis includes testing for lactate concentration. An important point to note with this test is that it is not performed prior to antimicrobial therapy. A study conducted with 78 patients with acute meningitis determined that all patients had CSF lactate concentrations greater than 4.2 mmol/L. Thus, lactate concentration could be used as a positive discriminative factor for bacterial meningitis with a sensitivity of 96% and a specificity of 100%. However, this test is not widely used to diagnose bacterial meningitis because it does not provide much diagnostic information [2].
Determination of C-reactive protein (CRP) concentration
C-reactive protein (CRP) is produced in the liver and is released six hours after an acute inflammatory reaction, which means CRP could provide a measure of immunity response after infection with meningitis. Patients with meningitis were tested for CRP concentration. Researchers concluded that CRP sensitivity ranged from 69-99% and specificity ranged from 28-99% [3]. However, because of the wide ranges, this measure for confirmed diagnosis is also not widely used.
Determination of procalcitonin concentration
Another measure for meningitis diagnosis might be the presence of procalcitonin. Researchers studied 59 children that had been hospitalized for meningitis and the procalcitonin concentrations were surprisingly high at a concentration greater than 5.0µg/L. The sensitivity of these results was 94% and the specificity was 100%. In adults, the serum concentrations were also tested with concentrations over ng/mL. Both sensitivity and specificity were up to 100% for procalcitonin concentration in adults [4]. These high sensitivity and specificity results provide a positive outlook on using procalcitonin concentration as a diagnosis measure of bacterial meningitis. However, the equipment used to test for procalcitonin concentration is not readily available in clinics, so it is not often used as a diagnostic tool to test for meningitis [4].
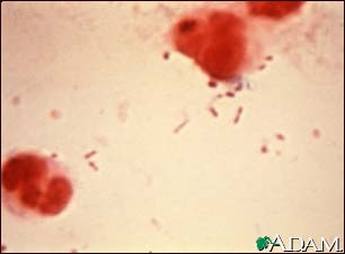
Gram stain depicting Haemophilus influenza [13].
Blood tests and imaging
Although the above measures are not often used due to low sensitivity and specificity measures or unavailable equipment in clinics, the following tests are most often used in patients that have a delayed lumbar puncture due concern of a intracranial, space-occupying lesion. An intracranial, space-occupying lesion is most often predicted if there is a “relative pressure gradient with a downward displacement of the cerebrum and brainstem that can cause brain herniation” [1]. Additionally, the lumbar puncture is delayed and blood tests also taken if the patient is experiencing short, convulsive seizures or if the patient has a history of seizures. Seizures pose a concern because they may be responsible for transient increases in intracranial pressure [1]. The following tests are commonly performed to test for meningitis:
Gram stain. A Gram stain is a method to distinguish between various types of bacteria by detecting if peptidoglycan is present in their cell wall. If peptidoglycan is present, then the bacteria is considered Gram positive, exhibiting a purple/blue color. Alternatively, a pink/red color means a Gram negative result. A Gram stain is important in clinical diagnoses because it can be performed faster than a culture and can help a patient receive timely treatment. The meningitis bacterium can be accurately detected in 60-90% of patients. A 103-105 CFU/mL will yield a positive Gram stain result in about 60% of the patients tested [1].
Latex agglutination. Latex agglutination are rapid tests that “utilize serum containing bacterial antibodies or commercially available antisera directed against the capsular poly saccharides of meningeal pathogens” [1]. Latex agglutination is not usually used as a primary decision mechanism for meningitis because there have been some false positive reports. However, latex agglutination is most useful for patients that have been pretreated with antibiotics and their Gram stain and CSF cultures results are negative. This allows clinicians to provide a correct positive diagnosis for patients that have already been on antimicrobial therapy [1].
Limulus lysate assay. Limulus lysate assay is most often used in patients that have exhibited a gram-negative result when meningitis is suspected. Limulus lysate is prepared from the amebocyte of the horseshoe crab, known as Limulus polyphemus, and provides a positive test result when there is endotoxin in the sample [1]. Though, this test is not commonly used first in response to suspected meningitis because the test cannot distinguish between specific gram-negative organisms. Thus, the Limulus lysate assay does not dismiss diagnosis of gram-negative meningitis, which is why it is only used when other tests yield false readings or inconclusive results [5].
Polymerase Chain Reaction. Polymerase Chain Reaction (PCR) is used to amplify DNA from patients with meningitis to see if common meningeal pathogens are present. PCR allows detection of pathogens to become easier, since the sample is amplified and provides a more sensitive analysis. More specifically, PCR delivers a sensitivity of 100%, a specificity of 98.2%, a positive predictive value of 98.2%, and a negative predictive value of 100%. Because of the high accuracy of this test, PCR may be significantly influential in decisions to begin or discontinue antimicrobial therapy [6].
Postmortem
The last method in which meningitis can be identified is through an autopsy. The medical examiner will often look for inflammation of the pia mater and arachnoid layers of the meninges to confirm meningitis was the cause of death. Another sign that meningitis was present at the time of death would be by inspection of the CSF. Most often neutrophil granulocytes are present in the CSF. Additionally, the base of the brain will most likely be covered in pus [7].
Although the above measures are not often used due to low sensitivity and specificity measures or unavailable equipment in clinics, the following tests are most often used in patients that have a delayed lumbar puncture due concern of a intracranial, space-occupying lesion. An intracranial, space-occupying lesion is most often predicted if there is a “relative pressure gradient with a downward displacement of the cerebrum and brainstem that can cause brain herniation” [1]. Additionally, the lumbar puncture is delayed and blood tests also taken if the patient is experiencing short, convulsive seizures or if the patient has a history of seizures. Seizures pose a concern because they may be responsible for transient increases in intracranial pressure [1]. The following tests are commonly performed to test for meningitis:
Gram stain. A Gram stain is a method to distinguish between various types of bacteria by detecting if peptidoglycan is present in their cell wall. If peptidoglycan is present, then the bacteria is considered Gram positive, exhibiting a purple/blue color. Alternatively, a pink/red color means a Gram negative result. A Gram stain is important in clinical diagnoses because it can be performed faster than a culture and can help a patient receive timely treatment. The meningitis bacterium can be accurately detected in 60-90% of patients. A 103-105 CFU/mL will yield a positive Gram stain result in about 60% of the patients tested [1].
Latex agglutination. Latex agglutination are rapid tests that “utilize serum containing bacterial antibodies or commercially available antisera directed against the capsular poly saccharides of meningeal pathogens” [1]. Latex agglutination is not usually used as a primary decision mechanism for meningitis because there have been some false positive reports. However, latex agglutination is most useful for patients that have been pretreated with antibiotics and their Gram stain and CSF cultures results are negative. This allows clinicians to provide a correct positive diagnosis for patients that have already been on antimicrobial therapy [1].
Limulus lysate assay. Limulus lysate assay is most often used in patients that have exhibited a gram-negative result when meningitis is suspected. Limulus lysate is prepared from the amebocyte of the horseshoe crab, known as Limulus polyphemus, and provides a positive test result when there is endotoxin in the sample [1]. Though, this test is not commonly used first in response to suspected meningitis because the test cannot distinguish between specific gram-negative organisms. Thus, the Limulus lysate assay does not dismiss diagnosis of gram-negative meningitis, which is why it is only used when other tests yield false readings or inconclusive results [5].
Polymerase Chain Reaction. Polymerase Chain Reaction (PCR) is used to amplify DNA from patients with meningitis to see if common meningeal pathogens are present. PCR allows detection of pathogens to become easier, since the sample is amplified and provides a more sensitive analysis. More specifically, PCR delivers a sensitivity of 100%, a specificity of 98.2%, a positive predictive value of 98.2%, and a negative predictive value of 100%. Because of the high accuracy of this test, PCR may be significantly influential in decisions to begin or discontinue antimicrobial therapy [6].
Postmortem
The last method in which meningitis can be identified is through an autopsy. The medical examiner will often look for inflammation of the pia mater and arachnoid layers of the meninges to confirm meningitis was the cause of death. Another sign that meningitis was present at the time of death would be by inspection of the CSF. Most often neutrophil granulocytes are present in the CSF. Additionally, the base of the brain will most likely be covered in pus [7].
Prevention
Behavioral

Meningococcal Vaccine [14].
Most often, meningitis is transmitted through respiratory secretions such as:
However, viral meningitis is more commonly spread through fecal contamination, especially in small children who have not been toilet trained. Although meningitis is usually spread through respiratory secretions, it can also be spread by surfaces, often surviving on hard surfaces for days. Symptoms first appear three to seven days after exposure. More information on behavioral transmission of meningitis can be found on the Centers for Disease Control’s website at: http://www.cdc.gov/meningitis/index.html.
Vaccination
Beginning in the 1980s, many countries include immunization against Haemophilus influenza type B as part or required childhood vaccines, which are most often needed prior to attending school. Additionally, routine vaccines also protect against Streptococcus pneumonia. This vaccine, known as pneumococcal conjugate vaccine (PCV), is active against seven types of pathogens that cause meningitis. Meningococcus vaccines also exist for groups A, C, W135, and Y to protect the public against meningitis. Another type of vaccine, known as Bacillus Calmette-Guerin has also been used to lower the risk of children developing tuberculous meningitis. However, Bacillus Calmetter-Guerin is not recommended for adults because of lessened effectiveness. Additionally, short-term antibiotics have also been proven to reduce the risk of meningitis [8].
- Kissing
- Sneezing
- Coughing
However, viral meningitis is more commonly spread through fecal contamination, especially in small children who have not been toilet trained. Although meningitis is usually spread through respiratory secretions, it can also be spread by surfaces, often surviving on hard surfaces for days. Symptoms first appear three to seven days after exposure. More information on behavioral transmission of meningitis can be found on the Centers for Disease Control’s website at: http://www.cdc.gov/meningitis/index.html.
Vaccination
Beginning in the 1980s, many countries include immunization against Haemophilus influenza type B as part or required childhood vaccines, which are most often needed prior to attending school. Additionally, routine vaccines also protect against Streptococcus pneumonia. This vaccine, known as pneumococcal conjugate vaccine (PCV), is active against seven types of pathogens that cause meningitis. Meningococcus vaccines also exist for groups A, C, W135, and Y to protect the public against meningitis. Another type of vaccine, known as Bacillus Calmette-Guerin has also been used to lower the risk of children developing tuberculous meningitis. However, Bacillus Calmetter-Guerin is not recommended for adults because of lessened effectiveness. Additionally, short-term antibiotics have also been proven to reduce the risk of meningitis [8].
Treatment
Antibiotics
Fluoroquinolone medication [15].
Antibiotics are commonly used to treat bacterial meningitis. Traditional antibiotics include vancomycin; however, vancomycin is used in conjunction with either ceftriaxone or cefotaxime in infants and children suspected of being infected with bacterial meningitis. Ceftriaxone and cefotaxime are recommended along with vancomycin in some adults as well [1]. Other types of antibiotics used to treat bacterial meningitis besides vancomycin include:
Cephalosporins. Third-generation cephalosporins have also been proved to be effective in treating meningitis, especially meningitis caused by aerobic gram-negative bacilli. More specifically, this bacterium is of the Escherichia coli or Klebsiella species. If given cephalosporins, 78-94% of patients recovered compared to 40-90% mortality of previous treatments, including aminoglycoside, with or without chloramphenicol [9]. Cefepime, a fourth-generation cephalosporin, has been used primarily in infants and children because it is generally considered safe and just as effective as third-generation cephalosporins [10].
Rifampin. Rifampin is another option in terms of antibiotic treatment for meningitis. Although rifampin cannot be used along due to significant bacterial resistance, it does distribute throughout the body, including in high concentrations in the CSF. Because of the significant bacterial resistance, rifampin must be used in combination with vancomycin or a third-generation cephalosporin [1].
Carbapenems. If patients do not respond to the more traditional treatment with vancomycin or are infected with gram-negative bacilli that produce extended-spectrum β-lactamases or hyperproduce β-lactamases, meropenem may be an effective treatment option. Meropenem is especially effective in patients that have meningitis caused by gram-negative bacteria that are resistant to previous medications listed above [11].
Fluoroquinolones. Fluoroquinolones are only used in multi-drug resistant gram-negative bacilli or when patients do not respond to traditional therapy with medications explained previously. Fluoroquinolones are not well tolerated by the body and therefore should only be prescribed once other drug therapies have proven to be ineffective [1].
Cephalosporins. Third-generation cephalosporins have also been proved to be effective in treating meningitis, especially meningitis caused by aerobic gram-negative bacilli. More specifically, this bacterium is of the Escherichia coli or Klebsiella species. If given cephalosporins, 78-94% of patients recovered compared to 40-90% mortality of previous treatments, including aminoglycoside, with or without chloramphenicol [9]. Cefepime, a fourth-generation cephalosporin, has been used primarily in infants and children because it is generally considered safe and just as effective as third-generation cephalosporins [10].
Rifampin. Rifampin is another option in terms of antibiotic treatment for meningitis. Although rifampin cannot be used along due to significant bacterial resistance, it does distribute throughout the body, including in high concentrations in the CSF. Because of the significant bacterial resistance, rifampin must be used in combination with vancomycin or a third-generation cephalosporin [1].
Carbapenems. If patients do not respond to the more traditional treatment with vancomycin or are infected with gram-negative bacilli that produce extended-spectrum β-lactamases or hyperproduce β-lactamases, meropenem may be an effective treatment option. Meropenem is especially effective in patients that have meningitis caused by gram-negative bacteria that are resistant to previous medications listed above [11].
Fluoroquinolones. Fluoroquinolones are only used in multi-drug resistant gram-negative bacilli or when patients do not respond to traditional therapy with medications explained previously. Fluoroquinolones are not well tolerated by the body and therefore should only be prescribed once other drug therapies have proven to be ineffective [1].
Steroids
Steroids, namely dexamethasone, have also been used in conjunction with the various antibiotics explained above. When used together with antibiotics, steroids significantly reduce the rate of mortality, severe hearing loss, and irreversible neurological injury in adolescents and adults (Assiri, Alasmari, Zimmerman, Baddour, Erwin & Tleyjeh, 2009). Steroids help reduce swelling associated with meningeal infection.
References
[1] Tunkel, A., Hartman, B., Kaplan, S., Kaufman, B., Roos, K., Scheld, W. M., & Whitley, R. (2004). Practice guidelines for the management of bacterial meningitis. Clinical Infectious Diseases, 39(9), 1267-1284. doi:10.1086/425368
[2] Leib SL, Boscacci R, Gratzl O, Zimmerli W. Predictive value of cerebrospinal fluid (CSF) lactate level versus CSF/blood glucose ratio for the diagnosis of bacterial meningitis following neurosurgery. Clinical Infectious Diseases. 1999; 29:69-74.
[3] Sormunen P, Kallio MJT, Kilpi T, Peltola H. C-reactive protein is useful in distinguishing Gram stain-negative bacterial meningitis from viral meningitis in children. The Journal of Pediatrics. 1999; 134:725-9.
[4] Schwarz S, Bertram M, Schwab S, et al. Serum procalcitonin levels in bacterial and abacterial meningitis. Critical Care Medicine 2000; 28:1828-32.
[5] Mylonakis E, Hohmann EL, Calderwood SB. Central nervous system infection with Listeria monocytogenes: 33 years' experience at a general hospital and review of 776 episodes from the literature. Medicine (Baltimore) 1998; 77:313-36.
[6] Spanos A, Harrell FE Jr, Durack DT. Differential diagnosis of acute meningitis: an analysis of the predictive value of initial observations. JAMA 1989; 262:2700-7.
[7] Warrell, David A; et al. (2003). Oxford Textbook of Medicine Volume One. Oxford. pp. 1115–29. ISBN 0-19-852787-X.
[8] Segal S, Pollard AJ (2004). "Vaccines against bacterial meningitis". British Medical Bulletin. 72 (1): 65–81. doi:10.1093/bmb/ldh041
[9] Fong IW, Tomkins KB (1985). Review of Pseudomonas aerugiosa meningitis with special emphasis on treatment with ceftazidime. Review of Infectious Diseases 7:604-612.
[10] Saez-Llorens X, Castano E, Garcia R, et al. Prospective randomized comparison of cefepime and cefotaxime for treatment of bacterial meningitis in infants and children. Antimicrobial Agents Chemotherapy. 1995; 39:937-40.
[11] Schonwald S, Geus I, Lisic M, et al. Ciprofloxacin in the treatment of gram-negative bacillary meningitis. American Journal of Medicine. 1989; 87:248-9.
[12] U.S. National Library of Medicine. (2011). Cerebral spinal fluid (CSF) collection [Image]. Retrieved from National Institutes of Health website: http://www.nlm.nih.gov/medlineplus/ency/article/003428.htm
[13] Healthline. (2011). Haemophilus influenza organism [Image]. Retrieved from http://www.healthline.com/adamimage?contentId=1-000680&id=2930
[14] Lord, J. (2010, May 30). VRM: Meningitis Vaccine To Be Forced On 7th Graders & All College Students – Full Analysis [Image]. Retrieved from http://vaccineresistancemovement.org/?p=4415
[15] James. (n.d.). Effect of Utilization Policies for Fluoroquinolones: DISCUSSION. Retrieved from http://www.advances-in-medicine.com/2010/12/effect-of-utilization-policies-for-fluoroquinolones-discussion.html#more-2149
[2] Leib SL, Boscacci R, Gratzl O, Zimmerli W. Predictive value of cerebrospinal fluid (CSF) lactate level versus CSF/blood glucose ratio for the diagnosis of bacterial meningitis following neurosurgery. Clinical Infectious Diseases. 1999; 29:69-74.
[3] Sormunen P, Kallio MJT, Kilpi T, Peltola H. C-reactive protein is useful in distinguishing Gram stain-negative bacterial meningitis from viral meningitis in children. The Journal of Pediatrics. 1999; 134:725-9.
[4] Schwarz S, Bertram M, Schwab S, et al. Serum procalcitonin levels in bacterial and abacterial meningitis. Critical Care Medicine 2000; 28:1828-32.
[5] Mylonakis E, Hohmann EL, Calderwood SB. Central nervous system infection with Listeria monocytogenes: 33 years' experience at a general hospital and review of 776 episodes from the literature. Medicine (Baltimore) 1998; 77:313-36.
[6] Spanos A, Harrell FE Jr, Durack DT. Differential diagnosis of acute meningitis: an analysis of the predictive value of initial observations. JAMA 1989; 262:2700-7.
[7] Warrell, David A; et al. (2003). Oxford Textbook of Medicine Volume One. Oxford. pp. 1115–29. ISBN 0-19-852787-X.
[8] Segal S, Pollard AJ (2004). "Vaccines against bacterial meningitis". British Medical Bulletin. 72 (1): 65–81. doi:10.1093/bmb/ldh041
[9] Fong IW, Tomkins KB (1985). Review of Pseudomonas aerugiosa meningitis with special emphasis on treatment with ceftazidime. Review of Infectious Diseases 7:604-612.
[10] Saez-Llorens X, Castano E, Garcia R, et al. Prospective randomized comparison of cefepime and cefotaxime for treatment of bacterial meningitis in infants and children. Antimicrobial Agents Chemotherapy. 1995; 39:937-40.
[11] Schonwald S, Geus I, Lisic M, et al. Ciprofloxacin in the treatment of gram-negative bacillary meningitis. American Journal of Medicine. 1989; 87:248-9.
[12] U.S. National Library of Medicine. (2011). Cerebral spinal fluid (CSF) collection [Image]. Retrieved from National Institutes of Health website: http://www.nlm.nih.gov/medlineplus/ency/article/003428.htm
[13] Healthline. (2011). Haemophilus influenza organism [Image]. Retrieved from http://www.healthline.com/adamimage?contentId=1-000680&id=2930
[14] Lord, J. (2010, May 30). VRM: Meningitis Vaccine To Be Forced On 7th Graders & All College Students – Full Analysis [Image]. Retrieved from http://vaccineresistancemovement.org/?p=4415
[15] James. (n.d.). Effect of Utilization Policies for Fluoroquinolones: DISCUSSION. Retrieved from http://www.advances-in-medicine.com/2010/12/effect-of-utilization-policies-for-fluoroquinolones-discussion.html#more-2149
